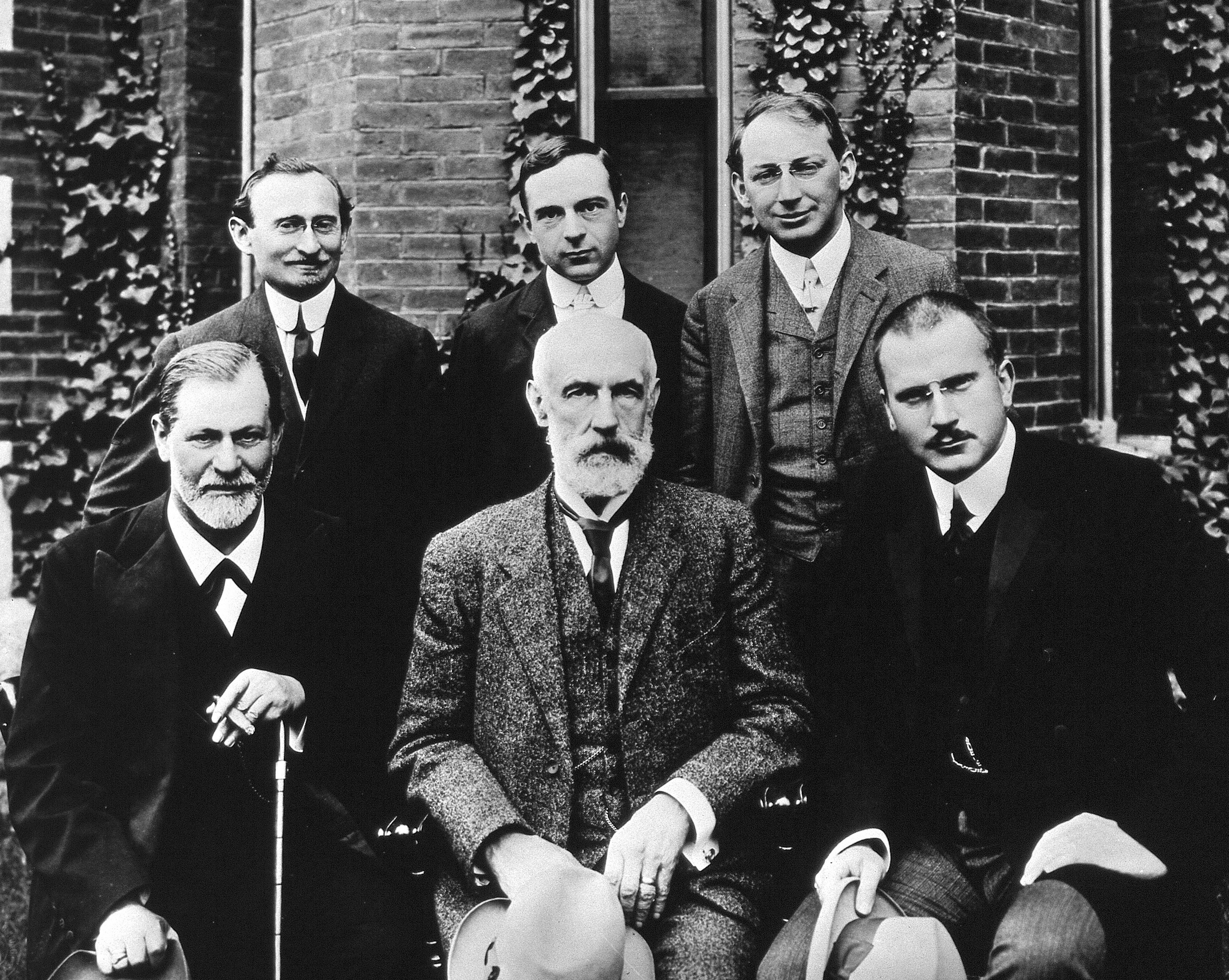
Group photo 1909 in front of Clark University. Front row: Sigmund Freud, G. Stanley Hall, Carl Jung; back row: Abraham A. Brill, Ernest Jones, Sandor Ferenczi.
Most importantly, and as outlined in this article, he came to believe that his patients' accounts of sexual abuse as children were truthful, having verified those accounts through other patients in the same family. This was a major reason for his eventual disputes with Sigmund Freud who had rejected the trauma model of Pierre Janet, which Freud termed the seduction theory, in favor of his own drive and fantasy theories.
Ferenczi was notable as a psychoanalyst for working with the most difficult of patients (where Freud had deemed these patients untreatable) and for developing a theory of more active intervention than is usual for psychoanalytic practice. During the early 1920s, criticizing Freud's "classical" method of neutral interpretation, Ferenczi collaborated with Otto Rank to create a "here-and-now" psychotherapy that, through Rank's personal influence, led the American Carl Rogers to conceptualize person-centered therapy (Kramer 1995) [1].
Relational analysts read Ferenczi as anticipating their own clinical emphasis on mutuality (intimacy), intersubjectivity, and the importance of the analyst's countertransference. Ferenczi's work has strongly influenced theory and praxis of the interpersonal-relational theory of American psychoanalysis, as typified by psychoanalysts at the William Alanson White Institute.
This paper was not published for many years after the original talk was given, and for 16 years following his death in 1933. In it he postulates a trauma theory based in relational failures, not in unconscious drives and fantasies. Many of the ideas in current relational theories of trauma can be found in this paper in crude form, but present nonetheless.
- Kramer, Robert (1995). The Birth of Client-Centered Therapy: Carl Rogers, Otto Rank, and 'The Beyond,' an article in Journal of Humanistic Psychology, 35(4), pp. 54–110.
Article Citation
Ferenczi, S. (1949). Confusion of the Tongues Between the Adults and the Child—(The Language of Tenderness and of Passion). International Journal of Psycho-Analysis, 30:225-230.
Translated by Michael Balint. Paper read at the Twelfth International Psycho-Analytical Congress, Wiesbaden, September, 1932. The original title of the paper as announced was 'The Passions of Adults and their Influence on the Sexual and Character Development of Children.' Published in Int. Z. f. Psa. (1933), 19, 5–15 and subsequently in Bausteine Zur Psychoanalyse, Vol. III. Berne, 1939.
Confusion of the Tongues Between the Adults and the Child—(The Language of Tenderness and of Passion)[1]
by Sándor Ferenczi
It was a mistake to try to confine the all too wide theme of the exogenous origin of character formations and neuroses within a Congress paper [2]. I shall, therefore, content myself with a short extract from what I would have had to say on that subject. Perhaps it will be best if I start by telling you how I have come to the problem expressed in the title of this paper. In the address given to the Viennese Psycho-Analytic Society on the occasion of Professor Freud's seventy-fifth birthday, I reported on a regression in technique (and partly also in the theory) of the neuroses to which I was forced by certain bad or incomplete results with my patients. By that I mean the recent, more emphatic stress on the traumatic factors in the pathogenesis of the neuroses which had been unjustly neglected in recent years. Insufficiently deep exploration of the exogenous factor leads to the danger of resorting prematurely to explanations—often too facile explanations—in terms of 'disposition' and 'constitution'.
The—I should like to say imposing—phenomena, the almost hallucinatory repetitions of traumatic experiences which began to accumulate in my daily practice, seemed to justify the hope that by this abreaction large quantities of repressed affects might obtain acceptance by the conscious mind and that the formation of new symptoms, especially when the superstructure of the affects had been sufficiently loosened by the analytic work, might be ended. This hope, unfortunately, was only very imperfectly fulfilled and some of my patients caused me a great deal of worry and embarrassment. The repetition, encouraged by the analysis, turned out to be too good. It is true that there was a marked improvement in some of the symptoms; on the other hand, however, these patients began to suffer from nocturnal attacks of anxiety, even from severe nightmares, and the analytic session degenerated time and again into an attack of anxiety hysteria. Although we were able to analyse conscientiously the threatening symptoms of such an attack, which seemed to convince and reassure the patient, the expected permanent success failed to materialize and the next morning brought the same complaints about the dreadful night, while in the analytic session, repetition of the trauma occurred. In this embarrassing position I tried to console myself in the usual way—that the patient had a much too forceful resistance or that he suffered from such severe repressions that abreaction and emergence into consciousness could only occur piecemeal. However, as the state of the patient, even after a considerable time, did not change in essentials, I had to give free rein to self-criticism. I started to listen to my patients when, in their attacks, they called me insensitive, cold, even hard and cruel, when they reproached me with being selfish, heartless, conceited, when they shouted at me: 'Help! Quick! Don't let me perish helplessly!' Then I began to test my conscience in order to discover whether, despite all my conscious good intentions, there might after all be some truth in these accusations. I wish to add that such periods of anger and hatred occurred only exceptionally; very often the sessions ended with a striking, almost helpless compliance and willingness to accept my interpretations. This, however, was so transitory that I came to realize that even these apparently willing patients felt hatred and rage, and I began to encourage them not to spare me in any way. This encouragement, too, failed to achieve much, for most of my patients energetically refused to accept such an interpretative demand although it was well supported by analytic material.
Gradually, then, I came to the conclusion that the patients have an exceedingly refined sensitivity for the wishes, tendencies, whims, sympathies and antipathies of their analyst, even if the analyst is completely unaware of this sensitivity. Instead of contradicting the analyst or accusing him of errors and blindness, the patients identify themselves with him; only in rare moments of an hysteroid excitement, i.e. in an almost unconscious state, can they pluck up enough courage to make a protest; normally they do not allow themselves to criticize us, such a criticism does not even become conscious in them unless we give them special permission or even encouragement to be so bold. That means that we must discern not only the painful events of their past from their associations, but also—and much more often than hitherto supposed—their repressed or suppressed criticism of us.
Here, however, we meet with considerable resistances, this time resistances in ourselves as well as in our patients. Above all, we ourselves must have been really well analysed, right down to 'rock bottom'. We must have learnt to recognize all our unpleasant external and internal character traits in order that we may be really prepared to face all those forms of hidden hatred and contempt that can be so cunningly disguised in our patients' associations.
This leads to the side issue—the analysis of the analyst—which is becoming more and more important. Do not let us forget that the deep-reaching analysis of a neurosis needs many years, while the average training analysis lasts only a few months, or at most, one to one and a half years [3]. This may lead to an impossible situation, namely, that our patients gradually become better analysed than we ourselves are, which means that although they may show signs of such superiority, they are unable to express it in words; indeed, they deteriorate into an extreme submissiveness obviously because of this inability or because of a fear of occasioning displeasure in us by their criticism.
A great part of the repressed criticism felt by our patients is directed towards what might be called professional hypocrisy. We greet the patient with politeness when he enters our room, ask him to start with his associations and promise him faithfully that we will listen attentively to him, give our undivided interest to his well-being and to the work needed for it. In reality, however, it may happen that we can only with difficulty tolerate certain external or internal features of the patient, or perhaps we feel unpleasantly disturbed in some professional or personal affair by the analytic session. Here, too, I cannot see any other way out than to make the source of the disturbance in us fully conscious and to discuss it with the patient, admitting it perhaps not only as a possibility but as a fact.
It is remarkable that such renunciation of the 'professional hypocrisy'—a hypocrisy hitherto regarded as unavoidable —instead of hurting the patient, led to a marked easing off in his condition. The traumatic-hysterical attack, even if it recurred, became considerably milder, tragic events of the past could be reproduced in thoughts without creating again a loss of mental balance; in fact the level of the patient's personality seemed to have been considerably raised.
Now what brought about this state of affairs? Something had been left unsaid in the relation between physician and patient, something insincere, and its frank discussion freed, so to speak, the tongue-tied patient; the admission of the analyst's error produced confidence in his patient. It would almost seem to be of advantage occasionally to commit blunders in order to admit afterwards the fault to the patient. This advice is, however, quite superfluous; we commit blunders often enough and one highly intelligent patient became justifiably indignant, saying: 'It would have been much better if you could have avoided blunders altogether. Your vanity, doctor, would like to make profit even out of your errors.'
The discovery and the solution of this purely technical problem revealed some previously hidden or scarcely noticed material. The analytical situation—i.e. the restrained coolness, the professional hypocrisy and—hidden behind it but never revealed—a dislike of the patient which, nevertheless, he felt in all his being—such a situation was not essentially different from that which in his childhood had led to the illness. When, in addition to the strain caused by this analytical situation, we imposed on the patient the further burden of reproducing the original trauma, we created a situation that was indeed unbearable. Small wonder that our effort produced no better results than the original trauma. The setting free of his critical feelings, the willingness on our part to admit our mistakes and the honest endeavour to avoid them in future, all these go to create in the patient a confidence in the analyst. It is this confidence that establishes the contrast between the present and the unbearable traumatogenic past, the contrast which is absolutely necessary for the patient in order to enable him to re-experience the past no longer as hallucinatory reproduction but as an objective memory. Suppressed criticisms felt by my patients, e.g. the discovery with uncanny clairvoyance, of the aggressive features of my 'active therapy', of the professional hypocrisy in the forcing of relaxation, taught me to recognize and to control the exaggerations in both directions. I am no less grateful to those of my patients who taught me that we are more than willing to adhere rigidly to certain theoretical constructions and to leave unnoticed facts on one side that would injure our complacency and authority. In any case, I learnt the cause of my inability to influence the hysterical explosions and this discovery eventually made success possible. It happened to me as it did to that wise woman whose friend could not be wakened from her narcoleptic sleep by any amount of shaking and shouting, to whom there came, suddenly, the idea of shouting 'Rock-a-bye baby'. After that the patient started to do everything she was asked to do. We talk a good deal in analysis of regressions into the infantile,but we do not really believe to what great extent we are right; we talk a lot about the splitting of the personality, but do not seem sufficiently to appreciate the depth of these splits. If we keep up our cool, educational attitude even vis-à-vis an opisthotonic patient, we tear to shreds the last thread that connects him to us. The patient gone off into his trance is a child indeed who no longer reacts to intellectual explanations, only perhaps to maternal friendliness; without it he feels lonely andabandoned in his greatest need, i.e. in the same unbearable situation which at one time led to a splitting of his mind and eventually to his illness; thus it is no wonder that the patient cannot but repeat now the symptom-formation exactly as he did at the time when his illness started.
I may remind you that patients do not react to theatrical phrases, but only to real sincere sympathy. Whether they recognize the truth by the intonation or colour of our voice or by the words we use or in some other way, I cannot tell. In any case, they show a remarkable, almost clairvoyant knowledge about the thoughts and emotions that go on in their analyst's mind. To deceive a patient in this respect seems to be hardly possible and if one tries to do so, it leads only to bad consequences.
Now allow me to report on some new ideas which this more intimate relation to my patients helped me to reach.
I obtained above all new corroborative evidence for my supposition that the trauma, especially the sexual trauma, as the pathogenic factor cannot be valued highly enough. Even children of very respectable, sincerely puritanical families, fall victim to real violence or rape much more often than one had dared to suppose. Either it is the parents who try to find a substitute gratification in this pathological way for their frustration, or it is people thought to be trustworthy such as relatives (uncles, aunts, grandparents), governesses or servants, who misuse the ignorance and the innocence of the child. The immediate explanation—that these are only sexual phantasies of the child, a kind of hysterical lying—is unfortunately made invalid by the number of such confessions, e.g. of assaults upon children, committed by patients actually in analysis. That iswhy I was not surprised when recently a philanthropically-minded teacher told me, despairingly, that in a short time he had discovered that in five upper class families the governesses were living a regular sexual life with boys of nine to eleven years old.
A typical way in which incestuous seductions may occur is this: an adult and a child love each other, the child nursing the playful phantasy of taking the rôle of mother to the adult. This play may assume erotic forms but remains, nevertheless, on the level of tenderness. It is not so, however, with pathological adults, especially if they have been disturbed in their balance and self-control by some misfortune or by the use of intoxicating drugs. They mistake the play of children for the desires of a sexually mature person or even allow themselves—irrespective of any consequences—to be carried away. The real rape of girls who have hardly grown out of the age of infants, similar sexual acts of mature women with boys, and also enforced homosexual acts, are more frequent occurrences than has hitherto been assumed.
It is difficult to imagine the behaviour and the emotions of children after such violence. One would expect the first impulse to be that of rejection, hatred, disgust and energetic refusal. 'No, no, I do not want it, it is much too violent for me, it hurts, leave me alone', this or something similar would be the immediate reaction if it would not be paralyzed by enormous anxiety. These children feel physically and morally helpless, their personalities are not sufficiently consolidated in order to be able to protest, even if only in thought, for the overpowering force and authority of the adult makes them dumb and can rob them of their senses. The same anxiety, however, if it reaches a certain maximum, compels them to subordinate themselves like automata to the will of the aggressor, to divine each one of his desires and to gratify these; completely oblivious of themselves they identify themselves with the aggressor. Through the identification, or let us say, introjection of the aggressor, he disappears as part of the external reality, and becomes intra- instead of extra-psychic; the intra-psychic is then subjected, in a dream-like state as is the traumatic trance, to the primary process, i.e. according to the pleasure principle it can be modified or changed by the use of positive or negative hallucinations. In any case the attack as a rigid external reality ceases to exist and in the traumatic trance the child succeeds in maintaining the previous situation of tenderness.
The most important change, produced in the mind of the child by the anxiety-fear-ridden identification with the adult partner, is the introjection of the guilt feelings of the adult which makes hitherto harmless play appear as a punishable offence.
When the child recovers from such an attack, he feels enormously confused, in fact, split—innocent and culpable at the same time—and his confidence in the testimony of his own senses is broken. Moreover, the harsh behaviour of the adult partner tormented and made angry by his remorse renders the child still more conscious of his own guilt and still more ashamed. Almost always the perpetrator behaves as though nothing had happened, and consoles himself with the thought: 'Oh, it is only a child, he does not know anything, he will forget it all.' Not infrequently after such events, the seducer
becomes over-moralistic or religious and endeavours to save the soul of the child by severity.
Usually the relation to a second adult—in the case quoted above, the mother—is not intimate enough for the child to find help there, timid attempts towards this end are refused by her as nonsensical. The misused child changes into a mechanical, obedient automaton or becomes defiant, but is unable to account for the reasons of his defiance. His sexual life remains undeveloped or assumes perverted forms. There is no need for me to enter into the details of neuroses and psychoses which may follow such events. For our theory this assumption, however, is highly important—namely, that the weak and undeveloped personality reacts to sudden unpleasure not by defence, but by anxiety-ridden identification and by introjection of the menacing person or aggressor. Only with the help of this hypothesis can I understand why my patients refused so obstinately to follow my advice to react to unjust or unkind treatment with pain or with hatred and defence. One part of their personalities, possibly the nucleus, got stuck in its development at a level where it was unable to use the alloplastic way of reaction but could only react in an autoplastic way by a kind of mimicry. Thus we arrive at the assumption of a mind which consists only of the Id and Super-Ego, and which therefore lacks the ability to maintain itself with stability in face of unpleasure—in the same way as the immature find it unbearable to be left alone, without maternal care and without a considerable amount of tenderness. Here we have to revert to some of the ideas developed by Freud a long time ago according to which the capacity for object-love must be preceded by a stage of identification.
I should like to call this the stage of passive object-love or of tenderness. Vestiges of object-love are already apparent here but only in a playful way in phantasies. Thus almost without exception we find the hidden play of taking the place of the parent of the same sex in order to be married to the other parent, but it must be stressed that this is merely phantasy; in reality the children would not want to, in fact they cannot do without tenderness, especially that which comes from the mother. If more love or love of a different kind from that which they need, is forced upon the children in the stage of tenderness, it may lead to pathological consequences in the same way as the frustration or withdrawal of love quoted elsewhere in this connection. It would lead us too far from our immediate subject to go into details of the neuroses and the character maldevelopments which may follow the precocious super-imposition of love, passionate and guilt loaded on an immature guiltless child. The consequence must needs be that of confusion of tongues, which is emphasized in the title of this address. Parents and adults, in the same way as we analysts, ought to learn to be constantly aware that behind the submissiveness or even the adoration, just as behind the transference of love, of our children, patients and pupils, there lies hidden an ardent desire to get rid of this oppressive love. If we can help the child, the patient or the pupil to give up the reaction of identification, and to ward off the over-burdening transference, then we may be said to have reached the goal of raising the personality to a higher level.
I should like to point briefly to a further extension of our knowledge made possible by these observations. We have long held that not only superimposed love but also unbearable punishments lead to fixations. The solution of this apparent paradox may perhaps now be possible. The playful trespasses of the child are raised to serious reality only by the passionate, often infuriated, punitive sanctions and lead to depressive states in the child who, until then, felt blissfully guiltless.
Detailed examination of the phenomena during an analytic trance teaches us that there is neither shock nor fright without some trace of splitting of personality. It will not surprise any analyst that part of the person regresses into the state of happiness that existed prior to the trauma—a trauma which it endeavours to annul. It is more remarkable that in the identification the working of a second mechanism can be observed, a mechanism the existence of which I, for one, have had but little knowledge. I mean the sudden, surprising rise of new faculties after a trauma, like a miracle that occurs upon the wave of a magic wand, or like that of the fakirs who are said to raise from a tiny seed, before our very eyes, a plant, leaves and flowers. Great need, and more especially mortal anxiety, seem to possess the power to waken up suddenly and to put into operation latent dispositions which, un-cathected, waited in deepest quietude for their development.
When subjected to a sexual attack, under the pressure of such traumatic urgency, the child can develop instantaneously all the emotions of mature adult and all the potential qualities dormant in him that normally belong to marriage, maternity and fatherhood. One is justified—in contradistinction to the familiar regression—to speak of a traumatic progression, of a precocious maturity. It is natural to compare this with the precocious maturity of the fruit that was injured by a bird or insect. Not only emotionally, but also intellectually, can the trauma bring to maturity a part of the person. I wish to remind you of the typical 'dream of the wise baby' described by me several years ago in which a newly-born child or an infant begins to talk, in fact teaches wisdom to the entire family. The fear of the uninhibited, almost mad adult changes the child, so to speak, into a psychiatrist and, in order to become one and to defend himself against dangers coming from people without self-control, he must know how to identify himself completely with them. Indeed it is unbelievable how much we can still learn from our wise children, the neurotics.
If the shocks increase in number during the development of the child, the number and the various kinds of splits in the personality increase too, and soon it becomes extremely difficult to maintain contact without confusion with all the fragments each of which behaves as a separate personality yet does not know of even the existence of the others. Eventually it may arrive at a state which—continuing the picture of fragmentation—one would be justified in calling atomization. One must possess a good deal of optimism not to lose courage when facing such a state, though I hope even here to be able to find threads that can link up the various parts.
In addition to passionate love and passionate punishment there is a third method of helplessly binding a child to an adult. This is the terrorism of suffering. Children have the compulsion to put to rights all disorder in the family, to burden, so to speak, their own tender shoulders with the load of all the others; of course this is not only out of pure altruism, but is in order to be able to enjoy again the lost rest and the care and attention accompanying it. A mother complaining of her constant miseries can create a nurse for life out of her child, i.e. a real mother substitute, neglecting the true interests of the
child.
I am certain—if all this proves true—that we shall have to revise certain chapters of the theory of sexuality and genitality. The perversions, for instance, are perhaps only infantile as far as they remain on the level of tenderness;if they become passionate and loaded with guilt, they are perhaps already the result of exogenous stimulation, of secondary, neurotic exaggeration. Also my theory of genitality neglected this difference between the phases of tenderness and of passion. How much of the sado-masochism in the sexuality of our time is due to civilization (i.e. originates only from introjected feelings of guilt) and how much develops autochtonously and spontaneously as a proper phase of organization, must be left for further research.
I shall be pleased if you would take the trouble to examine in thought and in your practice what I said to-day and especially if you would follow my advice to pay attention more than hitherto to the much veiled, yet very critical way of thinking and speaking to your children, patients and pupils and to loosen, as it were, their tongues. I am sure you will gain agood deal of instructive material.
APPENDIX
This train of thought points only descriptively to the tenderness of the infantile eroticism and to the passionate in the sexuality of the adult. It leaves open the problem of the real nature of this difference. Psycho-analysis willingly agrees with the Cartesian idea that passions are brought about by suffering, but perhaps will have to find an answer to the question of what it is that introduces the element of suffering, and with it sado-masochism, into the playful gratifications at the level of tenderness. The argument described above suggests that among others it is the guilt feelings that make the love-object in the erotic life of the adult an object of both loving and hating, i.e. of ambivalent emotions, while the infantile tenderness lacks as yet this schism. It is hatred that traumatically surprises and frightens the child while being loved by an adult, that changes him from a spontaneously and innocently playing being into a guilty love-automaton imitating the adult anxiously, self-effacingly. Their own guilt feelings and the hatred felt towards the seductive child partner fashion the love relation of the adults into a frightening struggle (primal scene) for the child. For the adult, this ends in the moment of orgasm, while infantile sexuality—in the absence of the 'struggle of the sexes'—remains at the level of forepleasure and knows only gratifications in the sense of 'saturation' and not the feelings of annihilation of orgasm. The 'Theory of Genitality' [4] that tries to found the 'struggle of the sexes' on phylogenesis will have to make clear this difference between the infantile-erotic gratifications and the hate-impregnated love of adult mating.
—————————————
1. Paper read at the Twelfth International Psycho-Analytical Congress, Wiesbaden, September, 1932.
2. The original title of the paper as announced was 'The Passions of Adults and their Influence on the Sexual and Character Development of Children.' Published in Int. Z. f. Psa. (1933), 19, 5–15 and subsequently in Bausteine Zur Psychoanalyse, Vol. III. Berne, 1939.
3. Written 1932.
4. Thalassa, 1938, New York. The Psycho-Analytic Quarterly Inc. (German original published in 1924.)
No comments:
Post a Comment